The coagulation cascade is responsible for secondary haemostasis. It occurs simultaneously to primary haemostasis and leads to development and maturation of the fibrin meshwork that stabilises the rapidly formed platelet plug.
The classical cascade is divided into three pathways: the intrinsic and extrinsic pathways, and the final common pathway. This distinction is arbitrary and originates from the historical laboratory methods used to asses coagulation.
 By Joe D - Own work, CC BY-SA 3.0, Link
By Joe D - Own work, CC BY-SA 3.0, Link
Intrinsic pathway
The contact activation (intrinsic) pathway is so named because of its initiation by contact with glass. Its component factors are XII, XI, IX, and VIII.
Extrinsic pathway
The extrinsic pathway, or tissue factor pathway, is the cascade of tissue factor and FVII.
Final common pathway
The final common pathway is the cascade following activation of FX by one of the tenase complexes. It ultimately leads to the cleavage of fibrinogen to fibrin, which is deposited and crosslinked at the platelet plug, stabilising it.
The modern cascade
The divisions of the coagulation cascade into separate pathways is arbitrary and technically inaccurate. It developed from the research and clinical laboratory methods used to study coagulation. The true interactions between clotting factors is complex and many factors further down the cascade positively reinforce coagulation. In vivo, secondary haemostasis is moved from its baseline activity towards, or away from, a procoagulant state by various interactions with inhibiting factors (not pictured below).
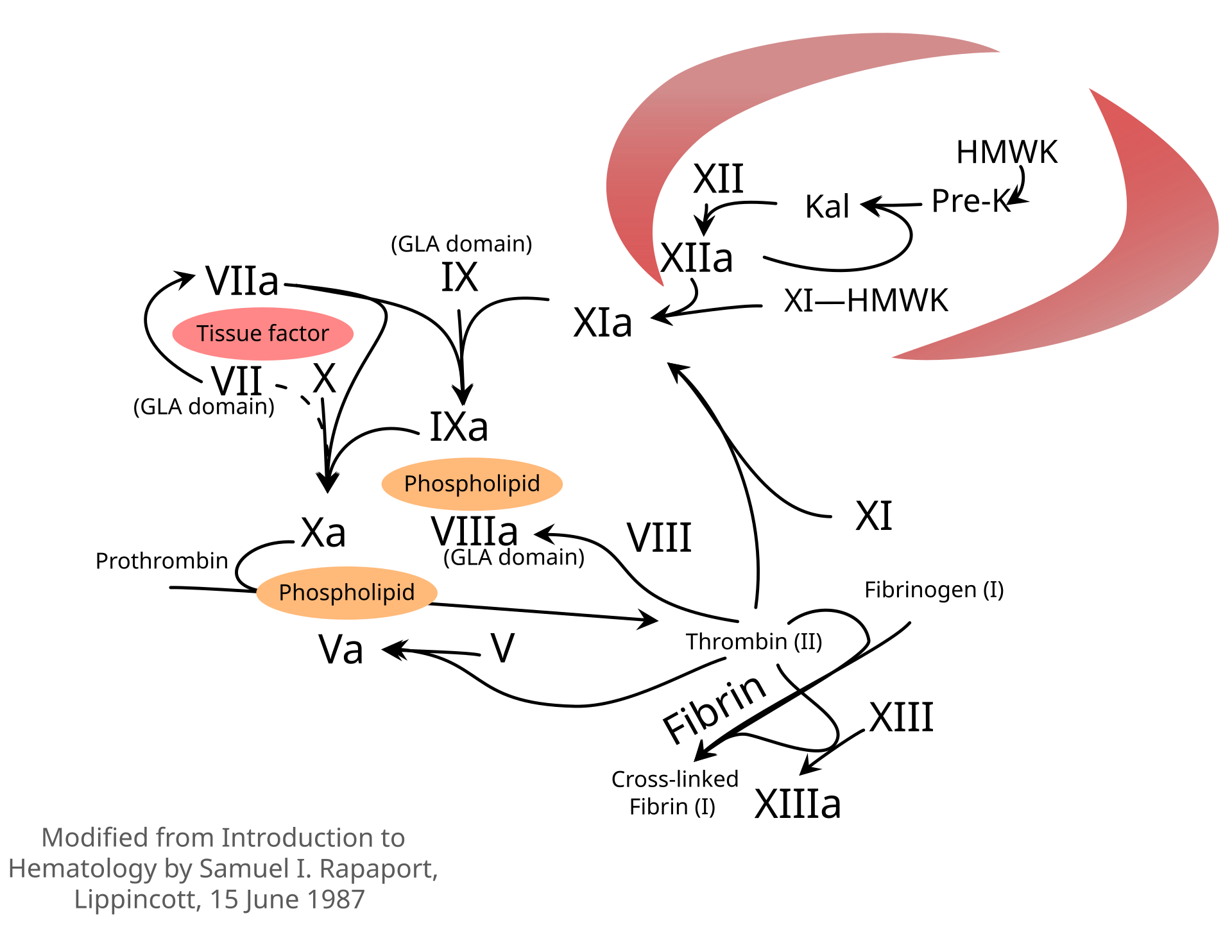 By Niels Olson - Own work, CC BY-SA 4.0, Link
By Niels Olson - Own work, CC BY-SA 4.0, Link